In 2020, I survived a suspected cardiac arrest and crashed my bike. An implantable cardioverter-defibrillator (ICD) — a small device placed under the skin of the chest to monitor and treat dangerous heart rhythms — was implanted as my safety net. Apart from greatly reducing my exercise levels due to the nature of my diagnosis, ARVC, I was living a relatively normal life. I even took part in Caledonia Etape on an Ebike in September 2021 — until I started noticing my neck swell and jugular veins pop out when I bent over, went swimming, lightly exerted, vacuumed or stirred a sauce for dinner.
The risk of SVC obstruction
While an ICD can be life-saving, there are potential risks associated with the implantation procedure. One of the most serious complications is superior vena cava (SVC) obstruction. The superior vena cava is a large vein that carries blood from the head, arms, and upper body to the heart. The ICD leads (wires) are positioned inside the SVC and can cause a blockage, leading to symptoms such as swelling in the face, neck, and arms, shortness of breath, and a blue or cyanotic appearance of the skin.
Neck gorging

My current ICD
I first began to experience some of these symptoms in October 2021 and after a clear CT and discharge from hospital A&E, I subsequently went into arrest and was shocked in December 2021 as can be seen on the video below.
https://twitter.com/damobird365/status/1470777671785267211?s=46&t=5j9uRy_XL5UDzkLeFkTfUA
SVC obstruction is a rare but potentially serious complication of ICD implantation. If SVC obstruction does occur, it can be treated with a procedure called Angioplasty / Venoplasty, in which a small balloon is used to open up the blocked vein, commonly via an incision in your groin, or with a surgical procedure to remove the obstruction. I had an attempted Angioplasty post arrest in December 2021 but the results were not perfect nor permanent. A second Angioplasty was attempted in September 2022 but was deemed too high risk during the operation.
Other risks
Other risks associated with ICD implantation include infection, bleeding, and injury to the heart or surrounding blood vessels. There is also a small risk of the device malfunctioning, which could lead to a failure to deliver therapy when it is needed or inappropriate shocks. Patients with an ICD need to be aware of magnetic fields that can disable their device. It does mean a pat down in an Airport for instance but you also need to be aware of magnets in your headphones or mobile phones, as often these are placed around your neck or in close proximity.
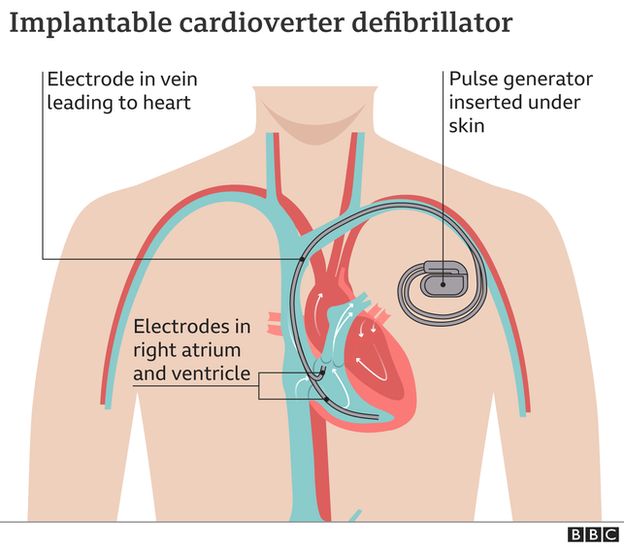
Image courtesy of BBC
Read more about footballer Christian Erikson here.
What other options are there?
An S-ICD, or subcutaneous implantable cardioverter-defibrillator, is a type of implantable device that is used to treat heart rhythm problems such as ventricular fibrillation and ventricular tachycardia. Unlike a traditional ICD, which is implanted under the skin of the chest and has leads (wires) that are placed into the heart, an S-ICD is implanted just under the skin of the chest and has leads that sit just under the skin, on the surface of the chest. The S-ICD does not require leads to be placed within the heart, making it a less invasive option for some patients.
S-ICD benefits, risks and limitations
One of the main benefits of an S-ICD is that it eliminates the risk of lead-related complications, such as lead fractures, infections or SVC obstruction, which can occur with traditional ICDs. Additionally, S-ICDs are less likely to cause damage to the heart or surrounding blood vessels during implantation. S-ICDs are also suitable for patients who are not suitable for traditional ICDs, for example, patients with congenital heart disease, or patients with limited venous access or previous cardiac surgery.
On the other hand, the S-ICD may not be suitable for all patients. For example, it may not be as effective as a traditional ICD in detecting certain types of heart rhythm problems, such as bradycardia (a slow heart rate) or providing pacing therapy. Additionally, the S-ICD may not be able to provide the same level of therapy as a traditional ICD in certain cases, such as cardioversion, which is a procedure that uses electrical energy to restart a normal heart rhythm.
Another potential risk associated with S-ICD is that the leads are situated just under the skin, which can make them more visible and may cause aesthetic concerns for some patients but at this point in my journey, I am desperate for a normal quality of life, that allows me to do some gardening, vacuum the house or go cycling with my kids or friends without feeling like a balloon is about to pop in my chest and head.
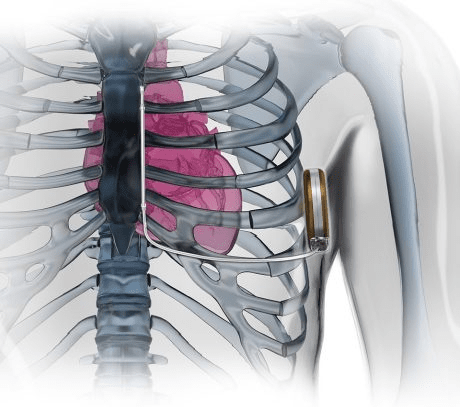
An S-ICD is approx 8cm x 6.5cm x 1.5cm in size and includes a lead and rod

My old ICD site

An incision for the lead and rod

The new S-ICD
Check out Footballer Charlie Wyke here who was fitted with an S-ICD and demonstrates where it’s been implanted.
An update on my situation
My surgery, originally scheduled for January 16th, was cancelled. Later, on January 24th, 2023, I went to the Accident and Emergency (A&E) department due to worsening symptoms. After a few days of being discharged, I went to Glasgow for an operation to remove my ICD and replace it with an S-ICD on February 2nd, 2023.
In the future, I will have an Angioplasty to address vein-related narrowing caused by natural tissue growth around the leads, but the tissue will remain after the extraction. This operation only dealt with the complications caused by the ICD, such as tissue growth over the leads and partial blockage. My heart disease remains the same after the surgery.
I hope that by sharing my experience, I can raise awareness among patients and healthcare professionals about the potential complications, risks, and benefits of ICDs and S-ICDs.